Τελευταία ενημέρωση: 11/12/2020
Συνοπτικός κατάλογος επιλεγμένων θεμάτων
Οδηγίες από την Ελληνική Πνευμονολογική Εταιρεία σχετικά με την σχετικά με τη διαχείριση ασθενούς ύποπτου ή επιβεβαιωμένου με COVID-19
Εξαιρετικές οδηγίες από την Ελληνική Πνευμονολογική Εταιρεία για τη χρήση μάσκας από το ευρύ κοινό. Περισσότερα για τις μάσκες προστασίας προσώπου.
Σε ποιο σημείο βρισκόμαστε στην ανάπτυξη εμβολίου
Παραγωγή αντισωμάτων (seroconversion) , Τεστ αντισωμάτων και Ανοσία στη νόσο COVID-19
Παραγωγή αντισωμάτων (seroconversion) , Τεστ αντισωμάτων και Ανοσία στη νόσο COVID-19
Tο φάρμακο remdesivir και ανασκόπηση της φαρμακευτικής θεραπείας της νόσου COVID-19
Η αχίλλειος πτέρνα στην αντιμετώπιση του SARS-CoV-2
Στρατηγική λήξης απομόνωσης (καραντίνας) ασθενών και με νόσο COVID-19 και των στενών επαφών τους από τον ΕΟΔΥ με βάση τις οδηγίες ECDC του Οκτωβρίου 2020
Τι καταφέραμε στην Ελλάδα!
Τι καταφέραμε στην Ελλάδα!
Επιδημιολογικά μοντέλα στη νόσο COVID-19
Χάρτες εξάπλωσης του SARS-CoV-2
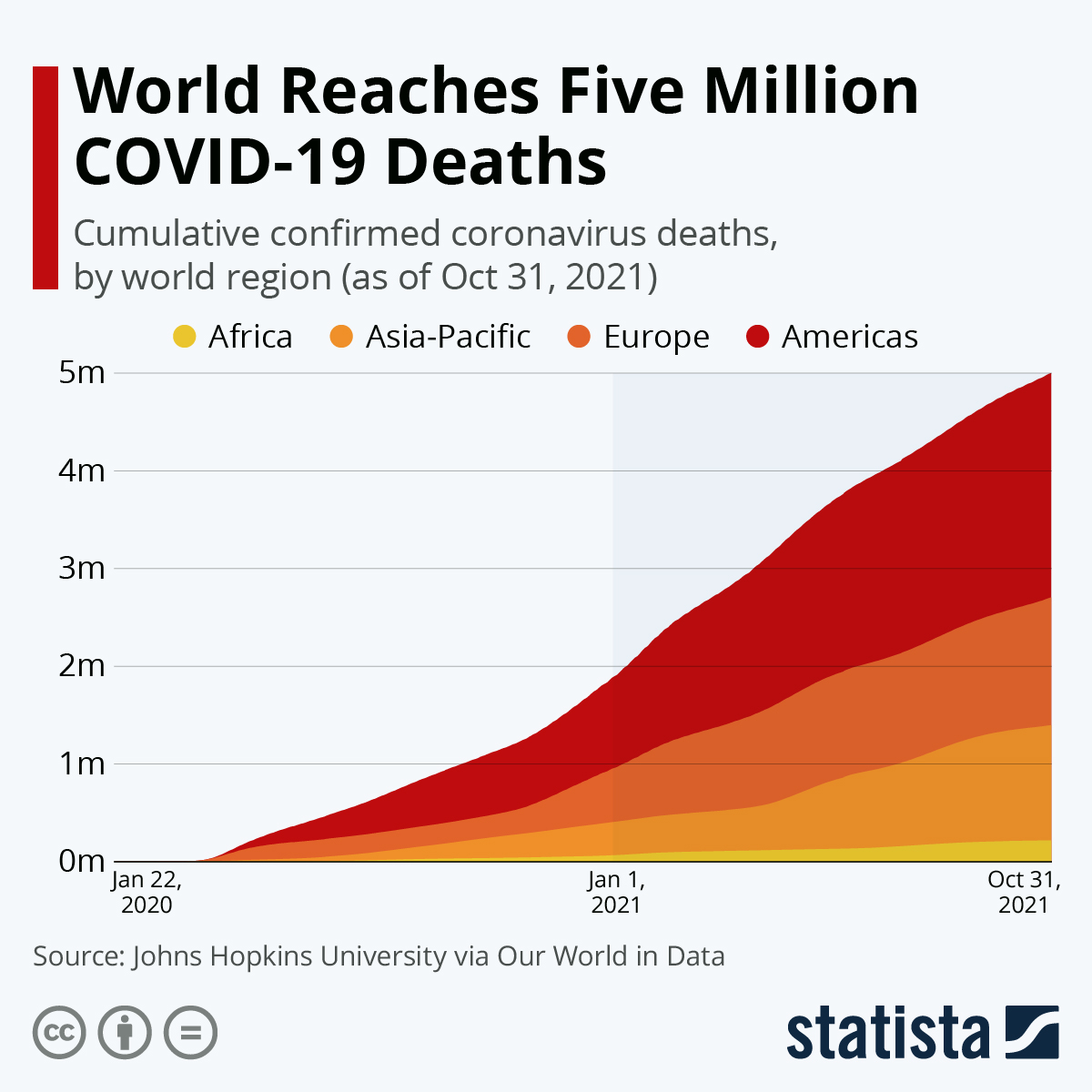
Το συνολικό τίμημα σε θανάτους ανά χώρα και ανά πληθυσμό
Παράγοντες κινδύνου για αυξημένη θνητότητα σε νοσηλευόμενους λόγω COVID-19 ασθενείς
Πρωτόκολλα προστασίας των αθλητών
Σχέδιο σταδιακής αποκλιμάκωσης περιοριστικών μέτρων και το αύριο της επιστροφής στην "κανονικότητα"
Σχέδιο σταδιακής αποκλιμάκωσης περιοριστικών μέτρων και το αύριο της επιστροφής στην "κανονικότητα"
Αναθεωρημένες συστάσεις για την αντιμετώπιση νοσούντων με Covid-19 ήπιας και μέσης βαρύτητας στο περιοδικό NEJM.
Patients may be infectious 1 to 3 days before symptom onset, and up to 40 to 50% of cases may be attributable to transmission from asymptomatic or presymptomatic people. Just before and soon after symptom onset, patients have high nasopharyngeal viral levels, which then fall over a period of 1 to 2 weeks. Patients may have detectable SARS-CoV-2 RNA on polymerase-chain-reaction (PCR) tests for weeks to months, but studies that detect viable virus and contact-tracing assessments suggest that the duration of infectivity is much shorter.
current expert recommendations support lifting isolation in most patients 10 days after symptom onset if fever has been absent for at least 24 hours (without the use of antipyretic agents) and other symptoms have decreased
Evaluation and management of Covid-19 depend on the severity of the disease. Patients with mild disease usually recover at home, whereas patients with moderate disease should be monitored closely and sometimes hospitalized.
Remdesivir and dexamethasone have demonstrated benefits in hospitalized patients with severe Covid-19, but in patients with moderate disease, dexamethasone is not efficacious (and may be harmful) and data are insufficient to recommend for or against routine use of remdesivir.
Θρομβοπροφύλαξη στη νόσο Covid-19: άρθρο στο περιοδικό NEJM. Συγκριτική παρουσίαση των τρεχουσών οδηγιών στο περιοδικό JAMA.
Φλεγμονή στη νόσο Covid-19: Cytokine storm και COVID-19 και Cytokine elevation in severe and critical COVID-19.
Ανάπτυξη εμβολίου για τη νόσο COVID-19: δημοσιευμένα δεδομένα
Τα θριαμβευτικά αποτελέσματα από την κλινική μελέτη mRNA εμβολίου φάσης 2/3 για τη νόσο COVID-19 των εταιρειών BioNTech και Pfizer: SPC του εμβολίου στο Ηνωμένο Βασίλειο, δημοσίευση στο περιοδικό NEJM και το συνοδευτικό editorial.
The vaccine BNT162b2 is a modified RNA that encodes a version of the SARS-CoV-2 spike protein containing mutations that lock the protein into a conformation that can induce neutralizing antibody responses. Early clinical trials showed that it could induce both humoral and cellular immunity.BNT162b2 a lipid nanoparticle–formulated nucleoside-modified RNA (modRNA) encoding the SARS-CoV-2 full-length spike, modified by two proline mutations to lock it in the prefusion conformationThe trial results are impressive enough to hold up in any conceivable analysis. This is a triumph. Most vaccines have taken decades to develop, but this one is likely to move from conception to large-scale implementation within a year.A two-dose regimen of BNT162b2 (30 μg per dose, given 21 days apart) was found to be safe and 95% effective against Covid-19. Only 8 cases of Covid-19 were seen in the vaccine group, as compared with 162 in the placebo group, for an overall efficacy of 95%.The cumulative incidence of Covid-19 cases over time among placebo and vaccine recipients begins to diverge by 12 days after the first dose, 7 days after the estimated median viral incubation period of 5 days, indicating the early onset of a partially protective effect of immunization.Nevertheless, in the interval between the first and second doses, the observed vaccine efficacy against Covid-19 was 52%, and in the first 7 days after dose 2, it was 91%, reaching full efficacy against disease with onset at least 7 days after dose 2Adverse events were largely consistent with vaccine reactogenicity, with mostly transient and mild local reactions such as injection-site pain and erythema; systemic reactions such as fever, fatigue, and adenopathy were uncommon.reactogenicity was generally mild or moderate, and reactions were less common and milder in older adults than in younger adults. Systemic reactogenicity was more common and severe after the second dose than after the first dose, although local reactogenicity was similar after the two doses. Severe fatigue was observed in approximately 4% of BNT162b2 recipients,Overall, reactogenicity events were transient and resolved within a couple of days after onset. Lymphadenopathy, which generally resolved within 10 days, is likely to have resulted from a robust vaccine-elicited immune response. The incidence of serious adverse events was similar in the vaccine and placebo groupsWhat happens to the inevitable large number of recipients who miss their second dose? How long will the vaccine remain effective? Does the vaccine prevent asymptomatic disease and limit transmission? And what about the groups of people who were not represented in this trial, such as children, pregnant women, and immunocompromised patients of various sorts?The logistic challenges of manufacturing and delivering a vaccine remain daunting. This vaccine, in particular, requires storage at −70°C.Τhe vaccine can be stored for up to 5 days at standard refrigerator temperatures once ready for use
Εταιρεία βιοτεχνολογίας Moderna (Cambridge, MA, USA): mRNA εμβόλιο:
Τα πρώιμα, ενθαρρυντικά αποτελέσματα από την κλινική μελέτη εμβολίου φάσης 1 για τη νόσο COVID-19: δημοσίευση στο περιοδικό NEJM.
Ωστόσο, υπάρχουν κάποιες επιφυλάξεις σχετικά με το φαινόμενο vaccine-associated immune enhancement:
Previous experience with veterinary coronavirus vaccines and animal models of SARS-CoV and MERS-CoV infection have raised safety concerns about the potential for vaccine-associated enhanced respiratory disease. These events were associated either with macrophage-tropic coronaviruses susceptible to antibody-dependent enhancement of replication or with vaccine antigens that induced antibodies with poor neutralizing activity and Th2-biased responses. Reducing the risk of vaccine-associated enhanced respiratory disease or antibody-dependent enhancement of replication involves induction of high-quality functional antibody responses and Th1-biased T-cell responses.
Oxford COVID Vaccine Trial Group σε συνεργασία με τη φαρμακευτική εταιρεία AstraZeneca : replication-deficient recombinant adenovirus-5-vectored εμβόλιο προερχόμενο από έναν αδενοϊό που προκαλεί νόσο στους χιμπατζηδες:
Τα ενθαρρυντικά αποτελέσματα από την κλινική μελέτη εμβολίου φάσεων 1 και 2: δημοσίευση στο περιοδικό Lancet.
The vaccine was safe and tolerated, with reduced reactogenicity when paracetamol was used prophylactically for the first 24 h after vaccination. A single dose elicited both humoral and cellular responses against SARS-CoV-2, with a booster immunisation augmenting neutralising antibody titres (the booster vaccine administered 28 days after the first dose). Reactogenicity was reduced after a second dose. Humoral responses to SARS-CoV-2 spike protein peaked by day 28 post prime and cellular responses were induced in all participants by day 14. Neutralising antibodies were induced in all participants after a second vaccine dose. After two doses, potent cellular and humoral immunogenicity was present in all participants studied.
prophylactic paracetamol to be administered before vaccination and participants were advised to continue with 1 g of paracetamol every 6 h for 24 h to reduce vaccine-associated reactions.Phase 3 trials are now underway in Brazil, South Africa, and the UK and will evaluate vaccine efficacy in diverse populations.
Φαρμακευτική εταιρεία CanSino Biologics (Wuhan, China), joint venture με φαρμακευτική εταιρεία Elli Lilly : non-replicating adenovirus type-5 (Ad5) vectored εμβόλιο:
Τα πρώιμα, ενθαρρυντικά αποτελέσματα από την πρώτη δημοσιευμένη κλινική μελέτη εμβολίου φάσης 1 για τη νόσο COVID-19: δημοσίευση στο περιοδικό Lancet.
Τα εξίσου ενθαρρυντικά αποτελέσματα από την κλινική μελέτη του ίδιου εμβολίου φάσης 2: δημοσίευση στο περιοδικό Lancet.
Our results suggest a single-dose immunisation schedule of Ad5-vectored COVID-19 vaccine at 5 × 1010 viral particles is an appropriate regimen for healthy adults. Compared with the younger population, we found older people to have a significantly lower immune response, but higher tolerability, to the Ad5-vectored COVID-19 vaccine. Therefore, an additional dose might be needed to induce a better immune response in the older population, and this will be evaluated in a phase 2b trial.
There are more than 100 candidate vaccines in development worldwide, among them at least eight have started or will soon start clinical trials. These include Moderna's mRNA COVID-19 vaccine and CanSino's non-replicating adenovirus type-5 (Ad5) vectored COVID-19 vaccine, which both entered phase 1 clinical trials on March 16, 2020; Inovio Pharmaceuticals' DNA vaccine for COVID-19, which entered trials on April 3, 2020; three inactive COVID-19 vaccines manufactured by Sinovac, Wuhan Institute of Biological Products, and Beijing Institute of Biological Products entered clinical trials in April, 2020, successively; University of Oxford's non-replicating chimpanzee adenovirus vectored vaccine ChAdOx1 nCoV-19, and BioNTech's mRNA COVID-19 vaccine also started trials in recent months.
Ανασκόπηση στο περιοδικό Lancet.
Ένας εξαιρετικός γραφικός οδηγός με τα είδη των υπό έρευνα πιθανών εμβολίων απέναντι στο νέο κορωνοϊό SARS-CoV-2 στο περιοδικό Nature !
Αντίστοιχο πολύ ενδιαφέρον άρθρο στο περιοδικό Economist :

A candidate which goes on to become a practical vaccine may be identified before the end of summer - perhaps more than one. But showing how well it works, finding any rare problems it may encounter, and manufacturing it in quantities large enough for the whole world will still take time.The world currently makes over 5bn doses of vaccine a year, of which roughly 1.5bn are seasonal-flu vaccines.
There are reports of some 86 candidate vaccines against SARS-CoV-2 being developedaround the world, taking a wide array of approaches. Three have already started phase I trials.One of these, made by CanSino Biologics, a Chinese biotechnology company, in collaboration with a unit of China’s Academy of Military Medical Sciences run by ChenWei, a major-general feted in the media, has been approved for phase II trials. The CanSino covid-19 vaccine that is reported to have entered phase II trials is a “recombinant vector” vaccine of this type, an adenovirus engineered to express the spike protein.
The most novel of the vaccines produced through genetic engineering are nucleic-acid vaccines. There are two such vaccines already in phase I trials. A number of other firms are not far behind.
Nucleic-acid vaccines have various advantages, according to their advocates. Their production is completely independent of viruses, or even cells, making contamination highly unlikely, and should in principle be easy to scale up. Last year cepi funded CureVac, a German biotech company, to develop an “rna printer” that would simply churn such vaccines out. If such production technologies work, there is a chance that they could be scaled up far faster than the techniques used for other vaccines.
The problem is that no rna or dna vaccine has yet been licensed for use in humans anywhere in the world. Adrian Hill, boss of Oxford University’s Jenner Institute, says describing them as vaccines is like saying you have a car without being able to say if it moves.
A particular safety worry for covid-19 vaccines is “antibody dependent enhancement”. During attempts to develop vaccines for SARS-CoV in the early 2000s, some laboratories saw test vaccines apparently improve the ability of the pathogen to enter cells.
Almost all the pharmaceutical industry’s vaccine-manufacturing know-how is concentrated in just four companies: GSK, Johnson & Johnson, Pfizer and Sanofi. And these four are generally wary of developing vaccines for pandemics, not least because developing vaccines for diseases that then vanish is even less profitable. Nevertheless, all four are contributing to covid-19 vaccine efforts. Despite such efforts, though, the ability to make vaccines will not be as widely distributed as the populations in need of them... mean fewer regular vaccines get made because, as Paul Stoffels, the managing director of Johnson & Johnson, confirms, “there is no excess capacity.”
An optimum strategy for using limited stocks of vaccine in a way that best benefits the world might see them devoted to populations at particular risk.
Σε ποιο σημείο βρισκόμαστε στην ανάπτυξη εμβολίου απέναντι στο νέο κορωνοϊό SARS-CoV-2: status report editorial στο περιοδικό Immunity Report :
Σε πλήρη αντιστοιχία με όσα αναφέρονται στην εξαιρετική κλινική ενημέρωση για τη νόσο COVID-2019 στο περιοδικό JAMA:The authors discuss therapeutic and prophylactic interventions for SARS-CoV-2 with a focus on vaccine development and its challenges. They provide an overview of vaccine production platforms and technologies and explain the time frames involved for development. These include preclinical and clinical trials, capacity to produce sufficient amounts according to Good Manufacturing Practice, administration procedures that will probably require additional doses (usually 3–4 weeks apart), and achievement of protective immunity 1–2 weeks after the second vaccination. The authors estimate availability no earlier than 6 months after the initiation of clinical trials and realistically not before another 12–18 months. They conclude that for SARS-CoV-2, vaccines will come too late to affect the first wave of this pandemic, but it is an absolute necessity for the additional waves or in a post-pandemic scenario in which SARS-CoV-2 continues to circulate as a seasonal virus.
When Will a Vaccine Be Available?
However, only 3 vaccine candidates are currently in phase 1 human trials: a messenger RNA vaccine and 2 adenovirus vector-based vaccines. The estimated timeline for availability of an initial vaccine is between early and mid-2021.Αντίστοιχες απόψεις εκφράζονται σε άρθρο στους New York Times, μαζί με μια ερμηνεία για τις υπεραισιόδοξες εκτιμήσεις που διατυπώνονται δημοσίως:
Why are all these research teams announcing such optimistic forηecasts when so many experts are skeptical about even an 18-month timeline? Perhaps because it’s not just the public listening — it’s investors, too. “These biotechs are putting out all these press announcements,” said Dr. Hotez. “You just need to recognize they’re writing this for their shareholders, not for the purposes of public health.”

Δεν είναι επιστροφή στην κανονικότητα! Αλλά η μετάβαση σε μια νέα εποχή, την πραγματικότητα μετά(;) το lock-down, διανθισμένη με την "παραδοσιακή" συνταγή της υπερρύθμισης (overregulation).. Και οι αβεβαιότητες, εδώ, μάλλον αυξάνονται!
Politicians in most countries are emphasising their willingness to follow science’s lead in matters concerning the pandemic. Their worry now must be that science has no lead to offer. (πηγή)
Με την ελπίδα και την προτροπή η χρήση μάσκας να μην οδηγήσει σε εφησυχασμό και ψευδές αίσθημα ασφαλείας από το κοινό! Όσο για το ιατρικό, νοσηλευτικό και παραϊατρικό προσωπικό τα παρακάτω λόγια περιγράφουν εύγλωττα τα διλήμματα...
Times like this can leave physicians stranded between our commitment to the community and responsibility to our families — a no man’s land where a colleague’s spare bed may be the closest approximation of home that we can find. (πηγή)
Σταχυολόγηση δημοσιεύσεων
Επιδημιολογικό μοντέλο το οποίο δείχνει ότι η επίδραση των κλιματολογικών συνθηκών στην εξάπλωση της πανδημικής νόσου COVID-19, και συγκεκριμένα η επικράτηση καλοκαιρινών θερμοκρασιών, είναι μάλλον μέτρια, καθώς η κύρια παράμετρος είναι ο συνδυασμός του βαθμού συλλογικής ανοσίας και της αποτελεσματικότητας των εφαρμοζόμενων περιοριστικών μέτρων: μελέτη στο περιοδικό Science.
While variations in weather may be important for endemic infections, during the pandemic stage of an emerging pathogen the climate drives only modest changes to pandemic size. While climate may play a role in modulating detailed aspects of the size and timescales of a pandemic outbreak within a particular location, population immunity is a much more fundamental driver of pandemic invasion dynamics. the key determinant of reduced peak incidence is the extent to which population immunity builds over the control period,both tropical and temperate locations should prepare for severe outbreaks of the disease and that summertime temperatures will not effectively limit the spread the infection. However, this does not mean the climate is not important in the longer term. Endemic cycles of the disease will likely be tied to climate factors and seasonal peaks may vary with latitudeThe climate plays a complex role in tuning the efficacy of potential control efforts, resulting in differential outcomes depending on location, however population susceptibility remains a fundamental driver. The timing of introduction and the efficacy of local control measures as well as factors such as population density and contact patterns could also shape future outcomes. Moreover, implementing control measures buys crucial time while vaccine and other treatments are developed.
Θεραπευτικοί αλγόριθμοι ΕΟΔΥ για την αντιμετώπιση εκτός νοσοκομείου ασθενών με εργαστηριακά επιβεβαιωμένη λοίμωξη από τον νέο κορωνοϊό-2019 SARS-CoV-2:
Η ουσιαστική διαφορά στην αναθεώρηση στης 30/4/2020 εντοπίζεται στους ενδιάμεσου κινδύνου ασθενείς, δηλαδή στην πλειονότητα των καταγεγραμμένων περιστατικών. Συγκεκριμένα, αναβαθμίζεται η σύσταση για παραπομπή σε νοσοκομείο αναφοράς, ενώ διαγράφηκε η σύσταση για εκτίμηση από τον "οικογενειακό ιατρό" της κλινικής εικόνας κατ΄οίκον με παρακολούθηση των αποτελεσμάτων της γενικής αίματος και της CRP, ορθώς κατά τη γνώμη του συντάκτη... Ωστόσο, παραμένει η μηχανιστική ερμηνεία και η μη αιτιολογητική διερεύνηση της υποξυγοναιμίας και της δύσπνοιας των ασθενών, χωρίς εξειδικευμένη πνευμονολογική εκτίμηση, με τον κίνδυνο της υπεραπόδοσης των κλινικών αυτών ευρημάτων στη νόσο COVID-19... Με άλλα λόγια, μια αναπνευστική ανεπάρκεια σε έναν ασθενή με θετική μοριακή δοκιμασία RT-PCR δεν σημαίνει απαραίτητα ότι η αναπνευστική ανεπάρκεια οφείλεται στη COVID-19!
Το πρόβλημα, όμως, παραμένει σταθερό στις διαδοχικές αυτές αναθεωρήσεις. Οι αλγόριθμοι αφήνουν ένα τεράστιο κενό, καθώς αναφέρονται στους ασθενείς μόνον που έχουν εργαστηριακή επιβεβαίωση της λοίμωξης, αλλά όχι στους ασθενείς που αποτελούν πιθανά περιστατικά λοίμωξης... Τη στιγμή που παραμένουν σε ισχύ ως οδηγίες από τον ΕΟΔΥ οι, μάλλον αυστηρές, ενδείξεις εργαστηριακού ελέγχου λοίμωξης από το νέο κορωνοϊό-2019 SARS-CoV-2.
Θεραπευτικοί αλγόριθμοι ΕΟΔΥ για τους ασθενείς που νοσηλεύονται στο νοσοκομείο με εργαστηριακά επιβεβαιωμένη λοίμωξη από τον νέο κορωνοϊό-2019 SARS-CoV-2:
Η ουσιαστική διαφορά στις διαδοχικές αναθεωρήσεις είναι η πρόταση έναρξης ανοσοτροποποιητικής ή και αντιικής θεραπείας στις βαρύτερες περιπτώσεις.
Ενδιαφέρουσα μελέτη στο περιοδικό Nature για την παραγωγή αντισωμάτων (seroconversion) στη νόσο COVID-2019:
the overall seroconversion rate was 96.8% (61/63) over the follow-up period. The proportion of patients with positive virus-specific IgG reached 100% approximately 17–19 days after symptom onset, while the proportion of patients with positive virus-specific IgM reached a peak of 94.1% approximately 20–22 days after symptom onset. Three types of seroconversion were observed: synchronous seroconversion of IgG and IgM (nine patients), IgM seroconversion earlier than that of IgG (seven patients) and IgM seroconversion later than that of IgG (ten patients). Both IgG and IgM titers plateaued within 6 days after seroconversion. Serological testing may be helpful for the diagnosis of suspected patients with negative RT–PCR results and for the identification of asymptomatic infections.However, a collection of the first serum sample as early as possible is required.
Remdesivir: προφάρμακο, ανάλογο της αδενοσίνης, με ευρεία αντιική δράση, χορηγούμενο ενδοφλεβίως, που δοκιμάστηκε ανεπιτυχώς έναντι του ιού Ebola. Μελέτη στο περιοδικό Lancet δείχνει ότι δεν βελτιώνει τη θνητότητα, την κλινική εικόνα και την κάθαρση του ιού στις σοβαρές μορφές της νόσου COVID-19, αν και είναι καλά ανεκτό. Ίσως, επιταχύνει οριακά την κλινική ανταπόκριση, όταν η χορήγησή του αρχίζει από τις πρώτες 10 ημέρες της συμπτωματολογίας. Αντίστοιχα είναι και τα προκαταρκτικά αποτελέσματα, αλλά και τα τελικά αποτελέσματα της μελέτης Adaptive COVID-19 Treatment Trial (ACTT) του NIAID των ΗΠΑ. Και επιβεβαιώνονται από τη μελέτη Solidarity του Παγκόσμιου Οργανισμού Υγείας σχετικά με τα προϋπάρχοντα, αναπροσανατολισμένα στη νόσο COVID-19 αντιικά φάρμακα:
These remdesivir, hydroxychloroquine, lopinavir, and interferon beta-1a regimens had little or no effect on hospitalized patients with Covid-19.
Ανασκόπηση της φαρμακευτικής θεραπείας της νόσου COVID-19 στο περιοδικό JAMA.

Ένα ανθρώπινο μονοκλωνικό αντίσωμα (47D11) ως πιθανή θεραπεία ή/και πρόληψη της νόσου COVID-19: μελέτη στο περιοδικό Nature Communications:
human monoclonal antibody that neutralizes SARS-CoV-2 (and SARS-CoV) in cell culture. This cross-neutralizing antibody targets a communal epitope on these viruses and may offer potential for prevention and treatment of COVID-19.
47D11 neutralizes SARS-CoV and SARS-CoV-2 through a yet unknown mechanism that is different from receptor-binding interference. Alternative mechanisms of coronavirus neutralization by receptor-binding domain (RBD)-targeting antibodies have been reported including spike inactivation through antibody-induced destabilization of its prefusion structure17, which may also apply for 47D11.
In conclusion, this is the first report of a (human) monoclonal antibody that neutralizes SARS-CoV-2. 47D11 binds a conserved epitope on the spike RBD explaining its ability to cross-neutralize SARS-CoV and SARS-CoV-2, using a mechanism that is independent of receptor-binding inhibition. This antibody will be useful for development of antigen detection tests and serological assays targeting SARS-CoV-2. Neutralizing antibodies can alter the course of infection in the infected host supporting virus clearance or protect an uninfected host that is exposed to the virus. Hence, this antibody—either alone or in combination—offers the potential to prevent and/or treat COVID-19, and possibly also other future emerging diseases in humans caused by viruses from the Sarbecovirus subgenus.
Η αχίλλειος πτέρνα στην αντιμετώπιση του SARS-CoV-2 είναι η μετάδοση από ασυμπτωματικούς, ολιγοσυμπτωματικούς και προσυμπτωματικούς ασθενείς: άρθρο στο περιοδικό NEJM.
asymptomatic persons are playing a major role in the transmission of SARS-CoV-2.A key factor in the transmissibility of Covid-19 is the high level of SARS-CoV-2 shedding in the upper respiratory tract, even among presymptomatic patients.
Ultimately, the rapid spread of Covid-19 across the globe, the clear evidence of SARS-CoV-2 transmission from asymptomatic persons, and the eventual need to relax current social distancing practices argue for broadened SARS-CoV-2 testing to include asymptomatic persons in prioritized settings, such as prisons and jails, enclosed mental health facilities, and homeless shelters, and to hospitalized inpatients. A new approach that expands Covid-19 testing to include asymptomatic persons residing or working in skilled nursing facilities needs to be implemented now. These factors also support the case for the general public to use face masks, when in crowded outdoor or indoor spaces.Αντιμετώπιση της αναπνευστικής ανεπάρκειας στη νόσο COVID-19: εξαιρετική κλινική ανασκόπηση στο περιοδικό JAMA.


NIH guidelines για την αντιμετώπιση της νόσου COVID-2019.
Υπάρχουν ακόμα αναπάντητα ερωτήματα για τα τεστ αντισωμάτων έναντι του νέου κορωνοϊού SARS-CoV-2: άρθρο στο περιοδικό Nature.
there are signs that the promises of COVID-19 antibody tests have been oversold, and their challenges underestimated. Kits have flooded the market, but most aren’t accurate enough to confirm whether an individual has been exposed to the virus. Furthermore, even reliable kits cannot indicate whether someone is immune to reinfection.
most kits have not undergone rigorous testing to ensure they’re reliable. Point-of-care tests are even less reliable than tests being used in labs.This is because they use a smaller sample of blood — typically from a finger prick — and are conducted in a less controlled environment than a lab, which can affect their performance
Another big question surrounding antibody tests is the extent to which being infected with a pathogen confers immunity to reinfection. To have protective immunity, the body needs to produce a certain type of antibody, called a neutralizing antibody, which prevents the virus from entering cells.
Even if it becomes clear that most people do develop neutralizing antibodies, most tests currently don’t detect them. And tests that do are more complex to develop and not widely available.
some politicians are pushing the idea that these tests be used to clear those with past COVID-19 infections to interact with others again, a so-called immunity passport. Researchers are trying to determine whether the antibodies detected by current kits can act as a proxy for protective immunity
Another complicating factor for immunity passports is that antibody tests can’t rule out that a person is no longer infectious. Viral RNA declines slowly after antibodies are detected in the blood. The presence of viral RNA could mean that the person is still shedding infectious virus.Συνέντευξη στο περιοδικό JAMA :
Marc Lipsitch of Harvard University predicts 50-70% of the global adult population could become infected with SARS-CoV-2. He discusses how prediction models are built and how they’re used and misused.Μία ενδιαφέρουσα υπόθεση προερχόμενη από την ιδιομορφία της "ισπανικής" γρίππης του 1918-1919: άρθρο στο περιοδικό Economist.
The influenza outbreak of 1918-19, known (unfairly to Spaniards) as the “Spanish” flu, for example, proved particularly harmful to those aged between 20 and 40.
One suggestion to explain what happened in 1918 is that those older than 40 tended to survive because they had acquired protective immunity from an earlier round of influenza to which younger generations had not been exposed. A second is that the more potent immune systems of the young overreacted to the 1918 virus for some reason, and that this triggered in them a cataclysmic, frequently fatal, immune response known as a cytokine storm.
Within the two-decade cohort of susceptible individuals in 1918 there was a particular spike in mortality among those exactly 28 years old.
Instead of these ideas Dr Gagnon and his colleagues support an alternative hypothesis, developed by Dennis Shanks of the Australian Army Malaria Institute, in Queensland, and John Brundage of the Armed Forces Health Surveillance Centre, in Maryland. This is that, in some circumstances, early exposure to a virus can harm subsequent immune responses rather than helping them.
Dr Shanks and Dr Brundage observed that in 1890, the birth year of those who were 28 in 1918, a different and less lethal strain of influenza, known as Russian flu, spread around the world. The immune systems of those exposed to Russian flu as newborn babies—a period of life when immune systems are especially attuned to learning about which pathogens are circulating—learnt about Russian flu all too well. As a consequence, when faced 28 years later with Spanish flu viruses they mounted the wrong response
Nor is the example of 1918 unique. According to Dr Gagnon, people who were themselves born during that epidemic showed increased vulnerability to the Hong Kong flu of 1968. And those born during the Asian flu of 1957 showed higher mortality in the face of swine flu in 2009.
Since all of his examples relate to influenza viruses, which are different beasts from coronaviruses, this is speculation.
Η κοινωνική αποστασιοποίηση είναι ένα προνόμιο, το οποίο δεν έχει ένα τμήμα του πληθυσμού που ζει κάτω από υποβαθμισμένες συνθήκες: άρθρο στο περιοδικό JAMA.
The most effective strategy known to reduce COVID-19 infection is social distancing, but herein lies a vexing challenge. Being able to maintain social distancing while working from home, telecommuting, and accepting a furlough from work but indulging in the plethora of virtual social events are issues of privilege. In certain communities these privileges are simply not accessible.
In Chicago, more than 50% of COVID-19 cases and nearly 70% of COVID-19 deaths involve black individuals, although blacks make up only 30% of the population.
Επιστροφή στην κανονικότητα από τη νόσο COVID-2019: άρθρο στο περιοδικό JAMA.
As part of pandemic preparedness, epidemiologists promote “containment strategies” designed to prevent community transmission. For coronavirus disease 2019 (COVID-19), countries like South Korea—an example of successful containment—had a coordinated governmental response, testing on a massive scale, and prompt contact tracing and quarantine. When disease outpaces containment, countries rely on "mitigation strategies". Mitigation relies on nonpharmaceutical interventions such as hand hygiene, travel restrictions, school closures, and social distancing.
As the US moves toward mid- to late May, there will be a staccato progression toward the restoration of a more normal life. The expected waves of recurrent disease will require management with intermittent short-term or “rolling” reclosures - triggered by sudden increases in hospital census data- all in an attempt to avoid another major surge of COVID-19 cases. Despite how challenging it is to answer the “when” question, addressing the “how” is no less daunting.
The cornerstone of the next phase will require massive testing, in 2 forms. First, serologic testing that detects immunoglobulins (IgM and IgG) specific for SARS-CoV-2 will provide estimates of population exposure. With an estimated reproduction number (R0) of 2 to 3, the benefits of herd immunity will occur when 50% to 66% of the population has already been infected, whether or not symptomatic. These population estimates could help guide the necessary level of vigilance and intervention.
Second, virologic polymerase chain reaction testing that detects active disease is important to effectively stop transmission. These tests must be easy to perform, quick to result, readily and equitably available outside of the health care setting, and inexpensive. Testing must be immediately accessible to anyone with any symptom suggestive of COVID-19, such as headache, fever, runny nose, cough, shortness of breath, diarrhea, malaise, or anosmia.
Whereas expansive testing is critical, testing alone is insufficient. Vital to any screening program is the action taken when a test result is positive. People identified with COVID-19 must be immediately informed, educated, isolated, and then their contacts efficiently identified, all in a manner sensitive to individual needs. Modeling studies suggest that to achieve effective control, contacts must be quarantined within 24 hours; SARS-CoV-2 transmission is simply too fast and manual contact-tracing too slow to curb epidemic spread. Rapid and effective tracing of contacts of infected individuals mandates creative app-based methods for immediate contact notification and quarantine.
At least some of the global spread of COVID-19 involved people with financial resources, such as cruise-goers and international flyers, but like many other epidemics, COVID-19 has quickly turned into a disease of the socially vulnerable.
Το κρίσιμο όριο για την επίτευξη συλλογικής ανοσίας (ανοσίας της αγέλης) στη νόσο COVID-19 ίσως είναι χαμηλότερα από την κλασική θεώρηση! Ωστόσο, η εφαρμογή αυστηρότερων μέτρων κοινωνικής αποστασιοποίησης ίσως οδηγεί όχι μόνο σε επιπεδωμένο πρώτο κύμα, αλλά και σε σοβαρότερο δεύτερο κύμα και τελικά αυξημένο αριθμό μολύνσεων: προσοχή στις μωβ καμπύλες των σχεδίων 1 και 2 της ενδιαφέρουσας μελέτης που δημοσιεύτηκε στο περιοδικό Science.
if R0 = 2.5 in an age-structured community with mixing rates fitted to social activity then the disease-induced herd immunity level can be around 43%, which is substantially less than the classical herd immunity level of 60% obtained through homogeneous immunization of the population.
An interesting observation is that the purple curve results in a higher overall fraction infected even though this scenario had more restrictions applied than the scenario of the yellow curve. This is because this epidemic was further from completion when sanctions were lifted.Only the curve corresponding to greatest preventive measures shows a severe second wave when restrictions are lifted. In most cases no (strong) second wave of outbreak occurs once preventive measures are lifted.
Οι περιορισμοί της στρατηγικής ιχνηλάτησης των κρουσμάτων στον έλεγχο της εξάπλωσης της νόσου COVID-19: άρθρο στο περιοδικό Lancet.
in most plausible outbreak scenarios, case isolation and contact tracing alone is insufficient to control outbreaks, and that in some scenarios even near perfect contact tracing will still be insufficient, and further interventions would be required to achieve control. Rapid and effective contact tracing can reduce the initial number of cases, which would make the outbreak easier to control overall. Effective contact tracing and isolation could contribute to reducing the overall size of an outbreak or bringing it under control over a longer time period.case isolation alone would be unlikely to control transmission within 3 months. Case isolation was more effective when there was little transmission before symptom onset and when the delay from symptom onset to isolation was short.Subclinical infection markedly decreased the probability of controlling outbreaks within 3 months. Higher presymptomatic transmission decreases the probability that the outbreaks were controlled, under all reproduction numbers and isolation delay distributions tested.In scenarios in which the reproduction number was 2.5, 15% of transmission occurred before symptom onset, and there was a short delay to isolation, at least 80% of infected contacts needed to be traced and isolated to give a probability of control of 90% or more.Preventing transmission by tracing and isolating a larger proportion of contacts, thereby decreasing the effective reproduction number, improved the number of scenarios in which control was likely to be achieved. However, these outbreaks required a large number of cases to be contact traced and isolated each week, which is of concern when assessing the feasibility of this strategy.
Πολύ ενδιαφέρον μοντέλο εξάπλωσης μετά την περίοδο της πανδημίας του νέου κορωνοϊού SARS-CoV-2 στο περιοδικό Science :
the total incidence of COVID-19 illness over the next five years will depend critically upon whether or not it enters into regular circulation after the initial pandemic wave, which in turn depends primarily upon the duration of immunity that SARS-CoV-2 infection imparts
Social distancing strategies could reduce the extent to which SARS-CoV-2 infections strain health care systems. Highly-effective distancing could reduce SARS-CoV-2 incidence enough to make a strategy based on contact tracing and quarantine feasible, as in South Korea and Singapore
Intermittent distancing may be required into 2022 unless critical care capacity is increased substantially or a treatment or vaccine becomes available.
given the economic burden that sustained distancing may impose, but we note the potentially catastrophic burden on the healthcare system that is predicted if distancing is poorly effective and/or not sustained for long enough
countries that have achieved this level of control of the outbreak should prepare for the possibility of substantial resurgences of infection and a return to social distancing measures, especially if seasonal forcing contributes to a rise in transmissibility in the winter. Moreover, a winter peak for COVID-19 would coincide with peak influenza incidence, further straining health care systems. One-time social distancing efforts may push the SARS-CoV-2 epidemic peak into the autumn, potentially exacerbating the load on critical care resources if there is increased wintertime transmissibility
Intermittent social distancing might maintain critical care demand within current thresholds, but widespread surveillance will be required to time the distancing measures correctly
New therapeutics, vaccines, or other interventions such as aggressive contact tracing and quarantine – impractical now in many places but more practical once case numbers have been reduced and testing scaled up– could alleviate the need for stringent social distancing to maintain control of the epidemic.
In the absence of such interventions, surveillance and intermittent distancing (or sustained distancing if it is highly effective) may need to be maintained into 2022, which would present a substantial social and economic burden.
Sustained, widespread surveillance will be needed both in the short term to effectively implement intermittent social distancing measures and in the long term to assess the possibility of resurgences of SARS-CoV-2 infection, which could occur as late as 2025 even after a prolonged period of apparent elimination
In the case of a 20-week period of social distancing with 60% reduction in R0, for example the resurgence peak size was nearly the same as the peak size of the uncontrolled epidemic: the social distancing was so effective that virtually no population immunity was built. The greatest reductions in peak size come from social distancing intensity and duration that divide cases approximately equally between peaks.
Of the temporary distancing scenarios, long-term (20-week), moderately effective (20%-40%) social distancing yields the smallest overall peak and total outbreak size.
For simulations with seasonal forcing, the post-intervention resurgent peak could exceed the size of the unconstrained epidemic, both in terms of peak prevalence and in terms of total number infected. Strong social distancing maintained a high proportion of susceptible individuals in the population, leading to an intense epidemic when R0 rises in the late autumn and winter. None of the one-time interventions was effective in maintaining the prevalence of critical cases below the critical care capacity. Preventing widespread infection during the summer can flatten and prolong the epidemic but can also lead to a high density of susceptible individuals who could become infected in an intense autumn wave. The observation that strong, temporary social distancing can lead to especially large resurgences agrees with data from the 1918 influenza pandemic in the United States , in which the size of the autumn 1918 peak of infection was inversely associated with that of a subsequent winter peak after interventions were no longer in place.
Intermittent social distancing could prevent critical care capacity from being exceeded. Due to the natural history of infection, there is an approximately 3-week lag between the start of social distancing and the peak critical care demand.
the overall duration of the SARS-CoV-2 epidemic could last into 2022, requiring social distancing measures to be in place between 25% (for wintertime R0 = 2 and seasonality; fig. S11A) and 75% (for wintertime R0 = 2.6 and no seasonality; fig. S9C) of that time.
the epidemic concluded by July 2022 and social distancing measures could be fully relaxed by early- to mid- 2021, depending again on the degree of seasonal forcing of transmission
Most crucially, serological studies could indicate the extent of population immunity, whether immunity wanes, and at what rate. In our model, this rate is the key modulator of the total SARS-CoV-2 incidence in the coming years
if serological data reveals the existence of many undocumented asymptomatic infections that lead to immunity, less social distancing may be required.
cross-immunity would lessen the intensity of SARS-CoV-2 outbreaks, though some speculate that antibody-dependent enhancement (ADE) induced by prior coronavirus infection may increase susceptibility to SARS-CoV-2 and exacerbate the severity of infection
Treatments or vaccines for SARS-CoV-2 would reduce the duration and intensity of social distancing required to maintain control of the epidemic. Treatments could reduce the proportion of infections that require critical care and could reduce the duration of infectiousness, which would both directly and indirectly (through a reduction in R0) reduce the demand for critical care resources. A vaccine would accelerate the accumulation of immunity in the population
Εξαιρετικό άρθρο άποψης για την ανοσία στον νέο κορωνοϊό-2019 SARS-CoV-2
After being infected with SARS-CoV-2, most individuals will have an immune response, some better than others. That response, it may be assumed, will offer some protection over the medium term — at least a year — and then its effectiveness might decline.
South Korea’s Centers for Disease Control and Prevention recently reported that 91 patients who had been infected with SARS-CoV-2 and then tested negative for the virus later tested positive again. If some of these cases were indeed reinfections, they would cast doubt on the strength of the immunity the patients had developed. An alternative possibility, which many scientists think is more likely, is that these patients had a false negative test in the middle of an ongoing infection, or that the infection had temporarily subsided and then re-emerged.
For now, it is reasonable to assume that only a minority of the world’s population is immune to SARS-CoV-2, even in hard-hit areas.
herd immunity to SARS-CoV-2 could be building faster than the commonly reported figures suggest.
Of 175 Chinese patients with mild symptoms of Covid-19, 70 percent developed strong antibody responses, but about 25 percent developed a low response and about 5 percent developed no detectable response at all. Mild illness, in other words, might not always build up protection. Similarly, it will be important to study the immune responses of people with asymptomatic cases of SARS-CoV-2 infection to determine whether symptoms, and their severity, predict whether a person becomes immune.
Whether some people are at greater or lesser risk of infection with SARS-CoV-2 because of a prior history of exposure to coronaviruses is an open question.
And then there is the question of immune enhancement: Through a variety of mechanisms, immunity to a coronavirus can in some instances exacerbate an infection rather than prevent or mitigate it. Guarding against enhancement will also be one of the biggest challenges facing scientists trying to develop vaccines for Covid-19
Διαδικασία λήψης ρινοφαρυγγικού επιχρίσματος: βίντεο και οδηγίες.στο περιοδικό NEJM. Και οι αντίστοιχες οδηγίες του CDC.
Οδηγίες του ECDC για εξιτήριο από το νοσοκομείο και τον τερματισμό της απομόνωσης των ασθενών με COVID-2019: ECDC Guidance for discharge and ending isolation in the context of widespread community transmission of COVID-19 – first update (8/4/2020). Μάλλον στην ίδια γραμμή με τις οδηγίες του CDC Discontinuation of Isolation for Persons with COVID-19 Not in Healthcare Settings , When to end home isolation (staying home).
23 επίκαιρες ερωτήσεις και απαντήσεις για τις διαγνωστικές εξετάσεις που γίνονται για τον νέο κορωνοϊό SARS-CoV-2 από το Ελληνικό Ινστιτούτο Παστέρ.
Αιρετική συνέντευξη του καθηγητή Didier Raoult, του υπέρμαχου της υδροξυχλωροκίνης:
On est devenus fous parce que ce sont les gens qui ne font pas de médecine qui parlent de médecine. La médecine c’est de pratiquer le soin au quotidien, à des gens qui sont malades, et leur donner un traitement. On ne leur dit pas " rentrez chez vous, et si vous n’arrivez plus à respirer venez à l’hôpital ". Ce n’est pas ça la médecine.
Τρελαθήκαμε, επειδή μιλούν για την ιατρική άνθρωποι που δεν ασκούν ιατρική. Η ιατρική είναι να δίνεις καθημερινή βοήθεια σε ασθενείς και να τους παρέχεις θεραπεία. Δεν τους λες "μείνετε σπίτι σας και αν δεν μπορείτε να αναπνεύσετε, ελάτε στο νοσοκομείο". Αυτό δεν είναι ιατρική!
Εξαιρετικό άρθρο - κλινική ενημέρωση για τη νόσο COVID-2019 στο περιοδικό JAMA:
Thus, it is important to emphasize that, depending on the clinical presentation, a negative RT-PCR result does not exclude COVID-19.
the median duration of IgM detection was 5 days (interquartile range, 3-6), while IgG was detected at a median of 14 days (interquartile range, 10-18) after symptom onset.
A fitted N95 respirator is the preferred type of medical mask for health care workers. Medical masks are also recommended for symptomatic individuals to prevent them from transmitting the virus.
A few changes may allow for easing restrictions: First, an aggressive program of testing to identify asymptomatic and mild cases combined with proactive contact tracing and early isolation as well as quarantine of contacts. Second, there must be a focus on reducing home-based transmission. In Wuhan, particularly after the initial phase, most transmissions occurred within households. While the CDC has published guidelines for preventing household transmission, it did not place enough emphasis on the importance of having the infected person always wear a mask. Third, even a treatment that only shortens an intensive care unit stay by 20% to 30% can have a substantial benefit on health system capacity.
When Will a Vaccine Be Available?
However, only 3 vaccine candidates are currently in phase 1 human trials: a messenger RNA vaccine and 2 adenovirus vector-based vaccines. The estimated timeline for availability of an initial vaccine is between early and mid-2021.
Κατευθυντήριες οδηγίες για αντιμετώπιση σοβαρά νοσούντων με Covid-19 στο περιοδικό JAMA και το editorial που το συνοδεύει
Συστάσεις για την αντιμετώπιση νοσούντων με Covid-19 σε επίπεδο μονάδας εντατικής θεραπείας στο περιοδικό Lancet.
Χαρακτηριστικά, συννοσηρότητα και έκβαση των νοσηλευόμενων ασθενών λόγω της νόσου COVID-2019 στην περιοχή της Νέας Υόρκης, σύμφωνα με την πλέον έγκυρη μέχρι τώρα δημοσίευση στο περιοδικό JAMA.
Ποια είναι τα χαρακτηριστικά των νοσηλευομένων σε ΜΕΘ λόγω της νόσου COVID-2019 στην Ιταλία, σύμφωνα με την πλέον έγκυρη μέχρι τώρα δημοσίευση στο περιοδικό JAMA
Ποια είναι τα κλινικά χαρακτηριστικά της νόσου COVID-2019 στην Κίνα, σύμφωνα με την πλέον έγκυρη μέχρι τώρα δημοσίευση στο περιοδικό NEJM
Η εμπειρία της Ισλανδίας: δημοσίευση στο περιοδικό NEJM
Μονοκλωνικά αντισώματα έναντι κυτταροκινών ως θεραπεία για την "πνευμονία" ή ακριβέστερα τον φλεγμονώδη καταρράκτη της νόσου COVID-2019: δημοσίευση στο περιοδικό Lancet Rheumatology
Παθητική ανοσοποίηση στη νόσο COVID-2019: θεραπεία με πλάσμα από ασθενείς που ανέρρωσαν. Δημοσίευση στο JAMA και το editorial (στο δρόμο για την χορήγηση υπεράνοσης ανoσοσφαιρίνης;)
Παράγοντες κινδύνου για θνητότητα των ασθενών με νόσο COVID-19 στην Κίνα: δημοσίευση στο Lancet.
Η μεγαλύτερη μέχρι τώρα αναφορά, προερχόμενη από την Κίνα, σε νεογέννητα από μητέρες με λοίμωξη Covid-2019: δημοσίευση στο JAMA
Ανασκόπηση για τον αυξημένο κίνδυνο στους καπνιστές σοβαρής νόσησης από τη νόσο COVID-19, νοσηλείας σε ΜΕΘ, διασωλήνωσης και θανάτου.
Χάρτης εξάπλωσης University of Washington HGIS Lab
Χάρτης εξάπλωσης Johns Hopkins University (έκδοση για κινητά)
Χάρτης εξάπλωσης Παγκόσμιου Οργανισμού Υγείας
Χάρτης εξάπλωσης ECDC, στην Ευρώπη και επιδημιολογικές καμπύλες ECDC
Χάρτης εξάπλωσης HealthMap του Boston Children’s Hospital
Χάρτης εξάπλωσης BNO news
Χάρτης εξάπλωσης Worldometer
Γραφική απεικόνιση των δεδομένων: Our World in Data
ECDC , An overview of the rapid test situation for COVID-19 diagnosis , Discharge criteria for confirmed COVID-19 cases from the hospital or end home isolation
CDC Discontinuation of Isolation for Persons with COVID-19 Not in Healthcare Settings , When to end home isolation (staying home)
Καθημερινή ενημέρωση και πηγή πληροφόρησης από την ERS.
Μάσκες προστασίας προσώπου
Σαφείς οδηγίες από την Ελληνική Πνευμονολογική Εταιρεία για την εξαίρεση από την χρήση μάσκας με αποδέκτες τους συντάκτες του άρθρου 5 του ΦΕΚ 3330/8-8-2020 τ.Β΄ και τους θιασώτες του γνωστού "κινήματος":
- Η αποφυγή της χρήσης μάσκας με τη γενική έννοια ‘’αναπνευστικοί ασθενείς’’ δεν έχει καμμιά εφαρμογή.
- Ειδικά για τους ασθενείς με χρόνια αναπνευστικά νοσήματα η χρήση μάσκας σε κλειστούς χώρους είναι ιδιαίτερα σημαντική μια και θεωρούνται άτομα υψηλού κινδύνου για σοβαρή νόσηση.
- Η χρήση μάσκας μπορεί εν τούτοις να επιφέρει σχετική αναπνευστική δυσφορία σε άτομα με χρόνια αναπνευστική ανεπάρκεια (που λαμβάνουν οξυγονοθεραπεία) ή με σοβαρές σπιρομετρικές διαταραχές.
- Σε αυτές μόνο τις περιπτώσεις, εφ΄ όσον κρίνεται αναγκαίο, δύναται να χορηγείται η κατάλληλη -σαφώς αιτιολογημένη- βεβαίωση από τον θεράποντα πνευμονολόγο.
- (θα πρέπει να προηγείται η) δοκιμή διαφορετικών τύπων μασκών για πιο άνετη χρήση (π.χ.αποφυγή υφασμάτινων και χρήση μασκών με βαλβίδα εκπνοής).
- Στις περιπτώσεις όπου η εφαρμογή οποιουδήποτε τύπου μάσκας δεν είναι εφικτή, θα πρέπει στον ασθενή να επεξηγούνται οι κίνδυνοι για την υγεία του που απορρέουν από τη μη χρήση μάσκας.
Άρα, η απάντηση στην τουλάχιστον "ατυχή" διατύπωση του άρθρου 5 του ΦΕΚ 3330/8-8-2020 τ.Β΄ για την εξαίρεση από την χρήση μάσκας, η οποία έδωσε λαβή στους θιασώτες του αντιεπιστημονικού "κινήματος" κατά της μάσκας, δεν είναι η έκδοση από το pipeline της ελληνικής γραφειοκρατίας ενός ακόμα ΦΕΚ ή ΚΥΑ αλλά η εξατομικευμένη εκτίμηση του κάθε ασθενούς από τον ειδικό επιστήμονα υγείας που είναι ο ειδικός πνευμονολόγος!
Ευτυχώς, η διατύπωση αυτή απαλείφθηκε στις οδηγίες του ΕΟΔΥ για τη λειτουργία των δημοτικών σχολείων!
Εξαιρετικές οδηγίες από την Ελληνική Πνευμονολογική Εταιρεία για τη χρήση μάσκας από το ευρύ κοινό. Μαζί με κάποιες επιφυλάξεις και επισημάνσεις...
οδηγίες και πλήρης κατάλογος για την προφύλαξη του υγειονομικού προσωπικού και το προσωπικό της βιομηχανίας από τον μεγαλύτερο κατασκευαστή παγκοσμίως...
Μάσκες προστασίας: προδιαγραφές και είδη
we strongly advocate universal use of face mask as a means of source control in public places during the COVID-19 pandemic. Extreme forms of social distancing is not sustainable, and complete lockdown of cities or even whole countries is extremely devastating to the economy. Universal masking in public complements social distancing and hand hygiene in containing or slowing down the otherwise exponential growth of the pandemic. A high degree of compliance will maximise the impact of universal masking in public. The global shortage of surgical and N95 respirators is a serious concern. In line with the recent recommedation by US CDC for healthy people to wear a cloth face cover in public, we strongly support the use of cloth masks as a simple, economic and sustainable alternative to surgical mask as a means of source control for general community use.
Συμβουλές για την οικογενειακή ζωή κατά την εποχή της κοινωνικής απομόνωσης στο σπίτι
Καταχωρημένες στο ClinicalTrials.gov κλινικές δοκιμές για την αντιμετώπιση της νόσου COVID-2019. Και η αντίστοιχη σύνοψη κλινικών μελετών από την ERS.
Αλγόριθμος ΕΟΔΥ: μια κριτική θεώρηση
(αναθεώρηση της 30/3/2020)
Στις 30/3/2020 αποσύρθηκε και αντικαταστάθηκε από την σελίδα του ΕΟΔΥ ο νέος θεραπευτικός αλγόριθμος για τους ασθενείς με λοίμωξη από τον νέο κορωνοϊό-2019 SARS-CoV-2. Συγκεκριμένα, στον ίδιο τόπο αναρτήθηκε ο αλγόριθμος για αντιμετώπιση όλων των ασθενών που προσέρχονται στα επείγοντα νοσοκομείου αναφοράς για τον SARS-CoV-2. Το πρόβλημα παραμένει και στην αναθεώρηση της 30/3/2020. Αφήνει ένα τεράστιο κενό, καθώς αναφέρεται στους ασθενείς μόνον που έχουν εργαστηριακή επιβεβαίωση της λοίμωξης, αλλά όχι στους ασθενείς που αποτελούν πιθανά κρούσματα.
Επίσης, στις 30/3/2020 αναρτήθηκαν στη σελίδα του ΕΟΔΥ οδηγίες για την αντιμετώπιση επιβεβαιωμένου κρούσματος Covid-2019 εκτός νοσοκομείου. Και αυτές οι οδηγίες προϋποθέτουν την εργαστηριακή επιβεβαίωση της λοίμωξης και δεν λαμβάνουν μέριμνα για τους ασθενείς που αποτελούν πιθανά κρούσματα. Επίσης, αναφέρεται χαρακτηριστικά:
Εάν ο ασθενής εμφανίζει αναπνευστική δυσχέρεια ή έχει κορεσμό Ο2≤93%, ανεξαρτήτως ομάδας κινδύνου εισάγεται στο νοσοκομείο
Κατά τη γνώμη του συντάκτη, η σύσταση αυτή είναι μηχανιστική, όχι εξατομικευμένη και μάλλον πλαδαρή. Υπάρχει ο κίνδυνος να οδηγήσει σε αθρόες εισαγωγές στα νοσοκομεία αναφοράς. Η δύσπνοια είναι υποκειμενική και μπορεί να αποδίδεται σε πλειάδα αιτίων. Το ίδιο και η υποοξυγοναιμία. Η εκτίμηση της κλινικής εικόνας και του status της αναπνευστικής λειτουργίας θα πρέπει να σε εξατομικευμένη βάση και πάντα σε σχέση με την προηγούμενη κατάσταση του ασθενούς. Ένας spO2=94% σε έναν νέο ασθενή με λευκό ιστορικό είναι, πιθανώς, δυσμενέστερο προγνωστικό σημείο από έναν spO2=91% σε έναν ασθενή που είναι παχύσαρκος και έχει χρόνια αποφρακτική πνευμονοπάθεια, σύνδρομο αποφρακτικής υπνικής άπνοιας και καρδιακή ανεπάρκεια.
Υπενθυμίζουμε ότι, παρά την αντίθετη παραίνεση του Παγκόσμιου Οργανισμού Υγείας περί "test, test, test" εκδόθηκαν νωρίτερα από τον ΕΟΔΥ οδηγίες ως ενδείξεις εργαστηριακού ελέγχου λοίμωξης από το νέο κορωνοϊό-2019 SARS-CoV-2.
Παρακάτω παρατίθενται κάποια σημεία για την αξία της αξονικής θώρακα στη νόσο Covid-2019.
Αλγόριθμος ΕΟΔΥ: μια κριτική θεώρηση
(μέχρι την αναθεώρηση της 30/3/2020)
(μέχρι την αναθεώρηση της 30/3/2020)
Aναρτήθηκε από τον ΕΟΔΥ νέος θεραπευτικός αλγόριθμος για τους ασθενείς με λοίμωξη από το νέο κορωνοϊό-2019 SARS-CoV-2, ως αναθεώρηση των προηγουμένων οδηγιών για τη θεραπεία των ασθενών.
Πάντως, κάποιες από τις προτεινόμενες θεραπείες έχουν αδύνατη τεκμηρίωση, όπως χαρακτηριστικά αναφέρεται στις κατευθυντήριες οδηγίες για αντιμετώπιση σοβαρά νοσούντων με Covid-19 στο περιοδικό JAMA...
There is insufficient evidence to issue a recommendation on use of any of the following: antiviral agents, recombinant interferons, chloroquine/hydroxychloroquine, or tocilizumab.
Ενώ ο αλγόριθμος από τον ΕΟΔΥ δεν κάνει αναφορά στα κορτικοειδή, τα οποία, πιθανώς, έχουν θέση, όχι στη μη επιπλεγμένη αναπνευστική ανεπάρκεια, αλλά στο σύνδρομο ARDS.
In adults receiving mechanical ventilation who do not have ARDS, routine use of systematic corticosteroids is suggested against (weak recommendation, LQE). In those with ARDS, use of corticosteroids is suggested (weak recommendation, LQE).Ο ίδιος αλγόριθμος προτείνει στην λήψη εμπειρικής αγωγής κατά της πνευμονίας της κοινότητας σε ασθενείς χωρίς αναπνευστική ανεπάρκεια και με φυσιολογική αξονική θώρακα !!!
Και αφήνει ένα τεράστιο κενό, καθώς αναφέρεται στους ασθενείς μόνον που έχουν εργαστηριακή επιβεβαίωση της λοίμωξης, ακόμα και αν αυτοί είναι ασυμπτωματικοί, αλλά όχι στους ασθενείς που αποτελούν πιθανά κρούσματα. Υπενθυμίζουμε ότι, ορθώς, κατά τη γνώμη του συντάκτη, και παρά την αντίθετη παραίνεση του Παγκόσμιου Οργανισμού Υγείας περί "test, test, test" εκδόθηκαν νωρίτερα από τον ΕΟΔΥ οδηγίες ως ενδείξεις εργαστηριακού ελέγχου λοίμωξης από το νέο κορωνοϊό-2019 SARS-CoV-2. Αυτές οι ενδείξεις βρίσκονται σε προφανή αναντιστοιχία με τον αλγόριθμο, περί εργαστηριακής διάγνωσης, ακόμα και σε ασυμπτωματικούς ασθενείς...
Αξίζει να επισημανθούν μερικά σημεία από το editorial στο περιοδικό JAMA που συνοδεύει τις κατευθυντήριες οδηγίες για αντιμετώπιση σοβαρά νοσούντων με Covid-19:
The panel is explicit about the need to intubate patients who require invasive mechanical ventilation. Even though this point may seem obvious, it was nonetheless important to emphasize. Otherwise, any tendency to limit the care of critically ill patients with COVID-19 on the basis of poor prognosis might quickly become a self-fulfilling prophecy.
Such caveats for rescue therapies in extremis may be interpreted as an obligation to try anything before transitioning to end-of-life care. However, that approach may not be desirable or practical during a pandemic, especially when resources are scarce, or when interventions are likely to do more harm than good.
many recommendations in favor of interventions, even though the recommendations are rated as weak because they lack supporting evidence. When prioritizing scarce resources, clinicians and health care systems will have to choose among options that have limited evidence to support them, regardless of which should be the initial options
recommendations for the use of concomitant broad-spectrum antibiotics may be impractical, and perhaps unwise, in some clinical settings
Η θέση της αξονικής θώρακα στη νόσο Covid-2019
Τι ισχύει για το ιικό φορτίο στον κορωνοϊό:
- Τα ευρήματα από τη νόσο Covid-2019 στην αξονική θώρακα (εικόνα ground glass, πυκνώσεις) είναι μη ειδικά. Η αξονική θώρακα δεν μπορεί να βοηθήσει στην διαφορική διάγνωση από άλλες μορφές ιογενούς πνευμονίας, μικροβιακής πνευμονίας της κοινότητας και μια μεγάλη ομάδα διαμέσων πνευμονιών μη λοιμώδους αιτιολογίας...
- Επομένως, η αξονική θώρακα έχει μικρή θετική προγνωστική αξία στη διάγνωση της νόσου Covid-2019: μία θετική αξονική δεν σημαίνει απαραίτητα νόσηση από τον SARS-CoV-2.
- Στην εξαιρετική περίπτωση (case study) του κρουαζιερόπλοιου Diamond Princess από τους 112 ασθενείς με, εργαστηριακά επιβεβαιωμένη με τη μοριακή δοκιμασία RT-PCR, λοίμωξη από τον SARS-CoV-2 μόλις το 61% είχαν ευρήματα στην αξονική. Από την άλλη πλευρά, το 20% των συμπτωματικών ασθενών με εργαστηριακά επιβεβαιωμένη νόσο Covid-2019 είχαν φυσιολογική αξονική θώρακα.
- Επομένως, η αξονική θώρακα έχει μικρή αρνητική προγνωστική αξία στη διάγνωση της νόσου Covid-2019: μία φυσιολογική αξονική δεν αποκλείει τη νόσηση από τον SARS-CoV-2.
- Η αξονική θώρακα δεν προσθέτει διαγνωστική αξία στη μοριακή δοκιμασία RT-PCR και δεν μπορεί να την υποκαταστήσει.
- Η αξονική θώρακα έχει μικρή αξία στη διάγνωση της νόσου Covid-2019. Η υπερεκτίμηση της αξίας της μπορεί να είναι επικίνδυνη και να δημιουργήσει ένα ψευδές αίσθημα ασφάλειας, καθώς η φυσιολογική αξονική δεν αποκλείει τη νόσηση από τον SARS-CoV-2.
- Επί κλινικής υποψίας νόσου Covid-2019, ανεξάρτητα από το αποτέλεσμα της αξονικής θώρακα, επιβάλλεται η απομόνωση του ασθενούς, μέχρι να επιβεβαιωθεί η διάγνωση με τη μοριακή δοκιμασία ή μέχρι να παρέλθει το προβλεπόμενο διάστημα απομόνωσης των 14 ημερών.
- Η αξονική θώρακα κατά την περίοδο της πανδημίας θα πρέπει να διενεργείται με παράλληλη σχολαστική τήρηση των οδηγιών ασφάλειας. Ακόμα, όμως, και με την τήρηση του πρωτοκόλλου το ιατρικό και νοσηλευτικό προσωπικό ή το ακτινολογικό εργαστήριο μπορεί να αποτελέσει εστία μόλυνσης.
- η μοριακή δοκιμασία με real-time RT-PCR δεν σχετίζεται πάντα με τη μεταδοτικότητα
- η δοκιμασία με RT-PCR πιθανώς παραμένει θετική 6-8 ημέρες μετά το τέλος της μεταδοτικής φάσης
- το τέλος της μεταδοτικής φάσης συμπίπτει χρονικά με το τέλος της θετικής καλλιέργειας του ιού στο δείγμα του ασθενούς
- η βιολογική δοκιμασία έχει το μειονέκτημα ότι δεν μπορεί να διακρίνει τις ενεργές μορφές του ιού από τις ανενεργές (νεκρές, αδρανοποιημένες από αντισώματα)
- η καλλιέργεια του βιολογικού δείγματος του ασθενούς για τον κορωνοϊό εν μέσω της πανδημίας δεν είναι εφικτό να εφαρμοστεί σε μεγάλη κλίμακα
- οι σοβαρά πάσχοντες ασθενείς με Covid-2019 που χρειάστηκαν μηχανικό αερισμό είχαν υψηλό ιικό φορτίο μετά το δεκαήμερο από την έναρξη των συμπτωμάτων
- αντίθετα, κάποιοι ασθενείς με Covid-2019 που παρουσίασαν όψιμη επιδείνωση της αναπνευστικής λειτουργίας είχαν αρνητική βιολογική δοκιμασία σε υλικό από στοματοφάρυγγα. Αυτό μπορεί να σημαίνει είτε τη μετανάστευση του ιικού φορτίου από το ανώτερο προς το κατώτερο αναπνευστικό είτε ότι η όψιμη επιδείνωση στο επίπεδο των πνευμόνων έχει ανοσολογική βάση, κάτι που ανοίγει σε κάποιες περιπτώσεις ασθενών ένα θεραπευτικό παράθυρο στα κορτικοειδή και στην ανοσοθεραπεία.
Η κινητική του ιικού φορτίου των ασθενών με νόσο COVID-19: είναι υψηλότερο κατά τις πρώτες ημέρες της συμπτωματολογίας, κάτι που επιβεβαιώνεται και από μία άλλη μελέτη στο NEJM.
Συνδυασμός lopinavir με ritonavir (εμπορική ονομασία: Kaletra)
Συνδυασμός lopinavir (ένα αντιικό φάρμακο, type 1 aspartate protease inhibitor έναντι του HIV) με ritonavir (ένας αναστολέας του κυτοχρώματος P450, με σκοπό την παράταση του χρόνου ημίσειας ζωής, ουσιαστικά του χρόνου δράσης δηλαδή, του lopinavir) (εμπορική ονομασία: Kaletra), ως επιπρόσθετη θεραπεία (add-on) στους σοβαρά πάσχοντες ασθενείς με Covid-19:
η μελέτη της οποίας τα αποτελέσματα δημοσιεύτηκαν στο NEJM απέτυχε να δείξει όφελος ως προς την θνητότητα, την εξέλιξη της κλινικής πορείας της νόσου και το ιικό φορτίο. Επιπλέον, οι ασθενείς που έλαβαν τον συνδυασμό εμφάνισαν συχνότερα σοβαρές παρενέργειες από το γαστρεντερικό σύστημα, μέχρι σημείου πρόωρης διακοπής της αγωγής.


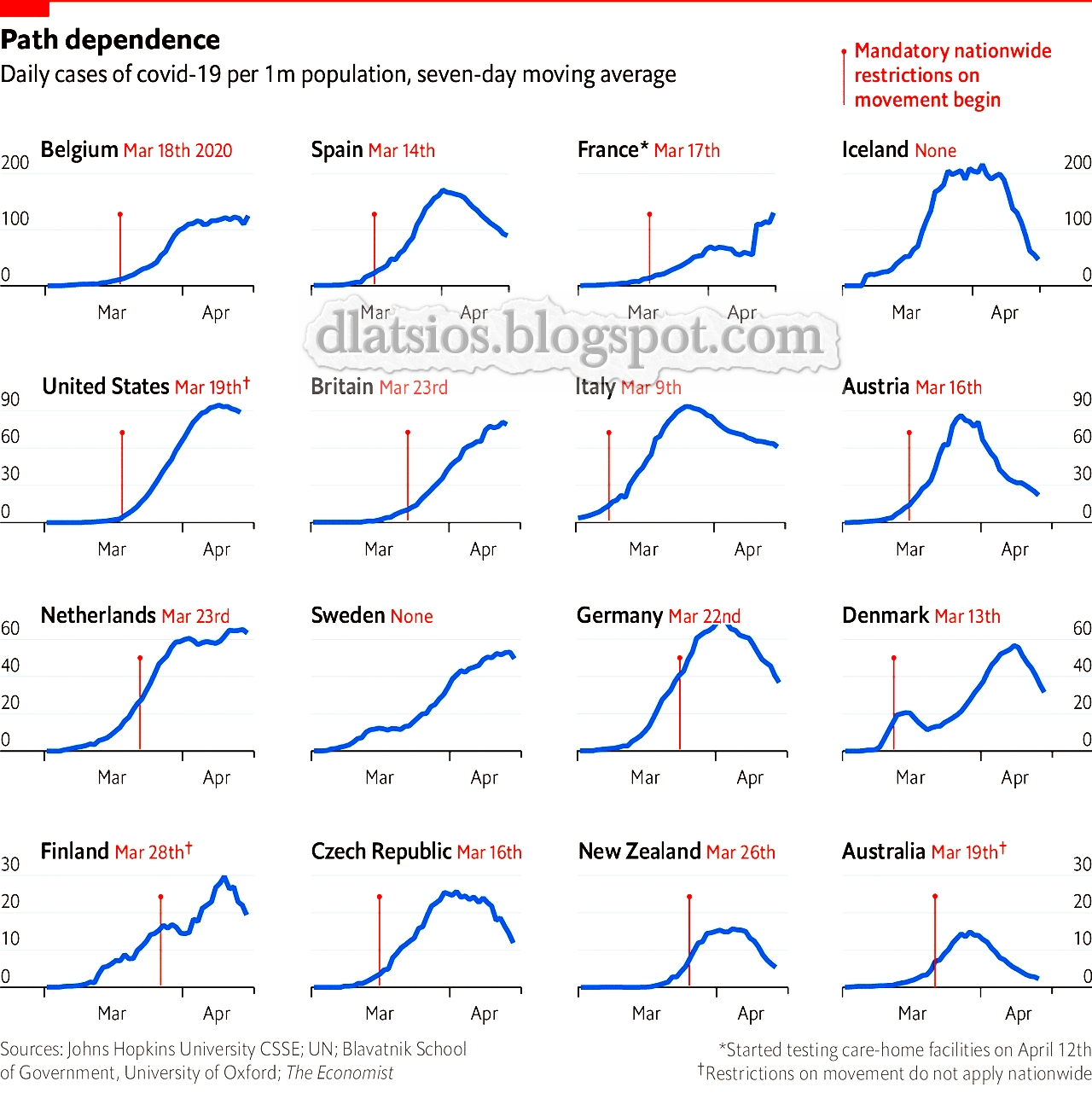

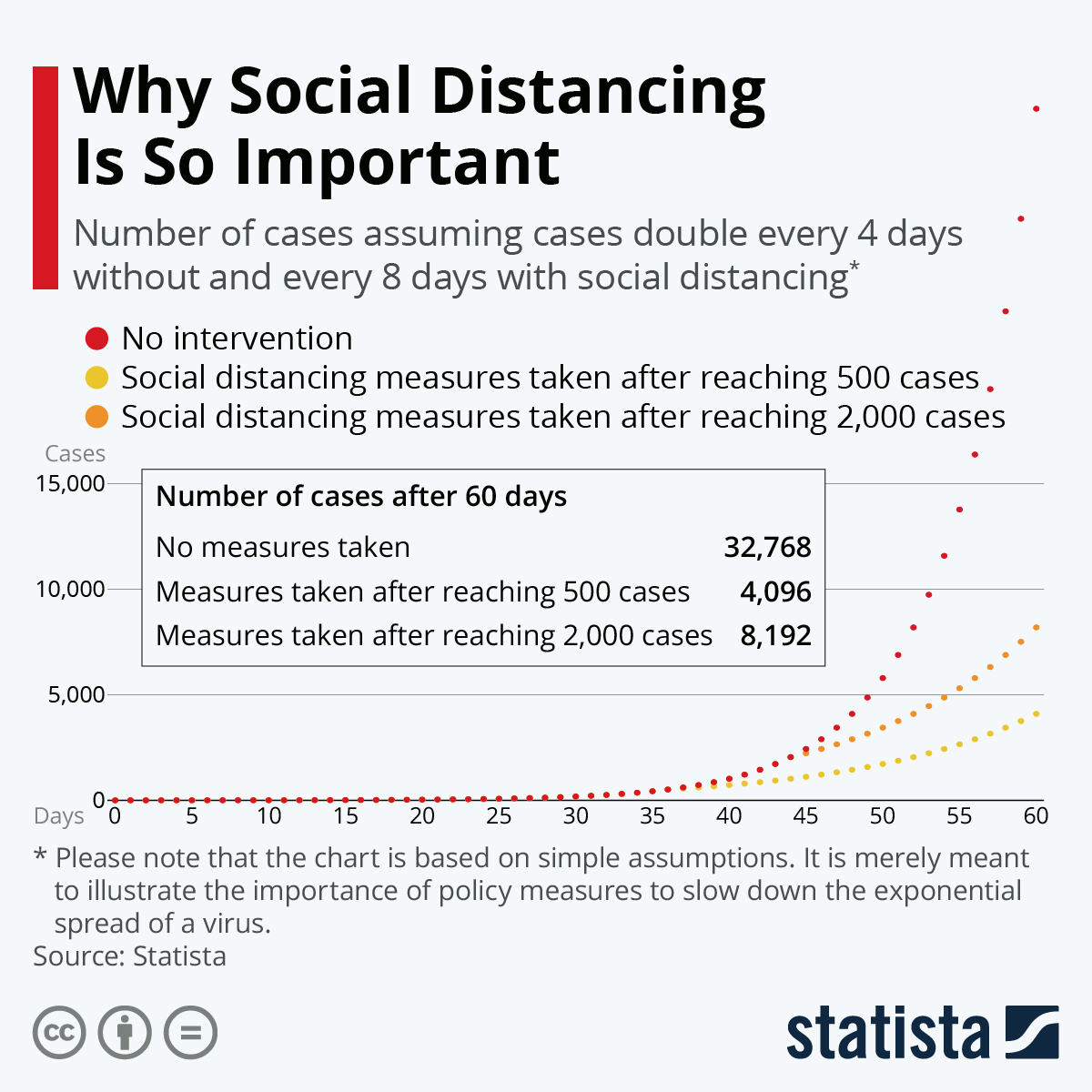
η σημασία της έγκαιρης εφαρμογής της
(ή πως να μην οδηγηθούμε στο forget lockdown, we are going into meltdown του NHS της Αγγλίας)
(ή πως να μην οδηγηθούμε στο forget lockdown, we are going into meltdown του NHS της Αγγλίας)
Η ημερήσια εξέλιξη των θανάτων στις περισσότερο πληττόμενες χώρες
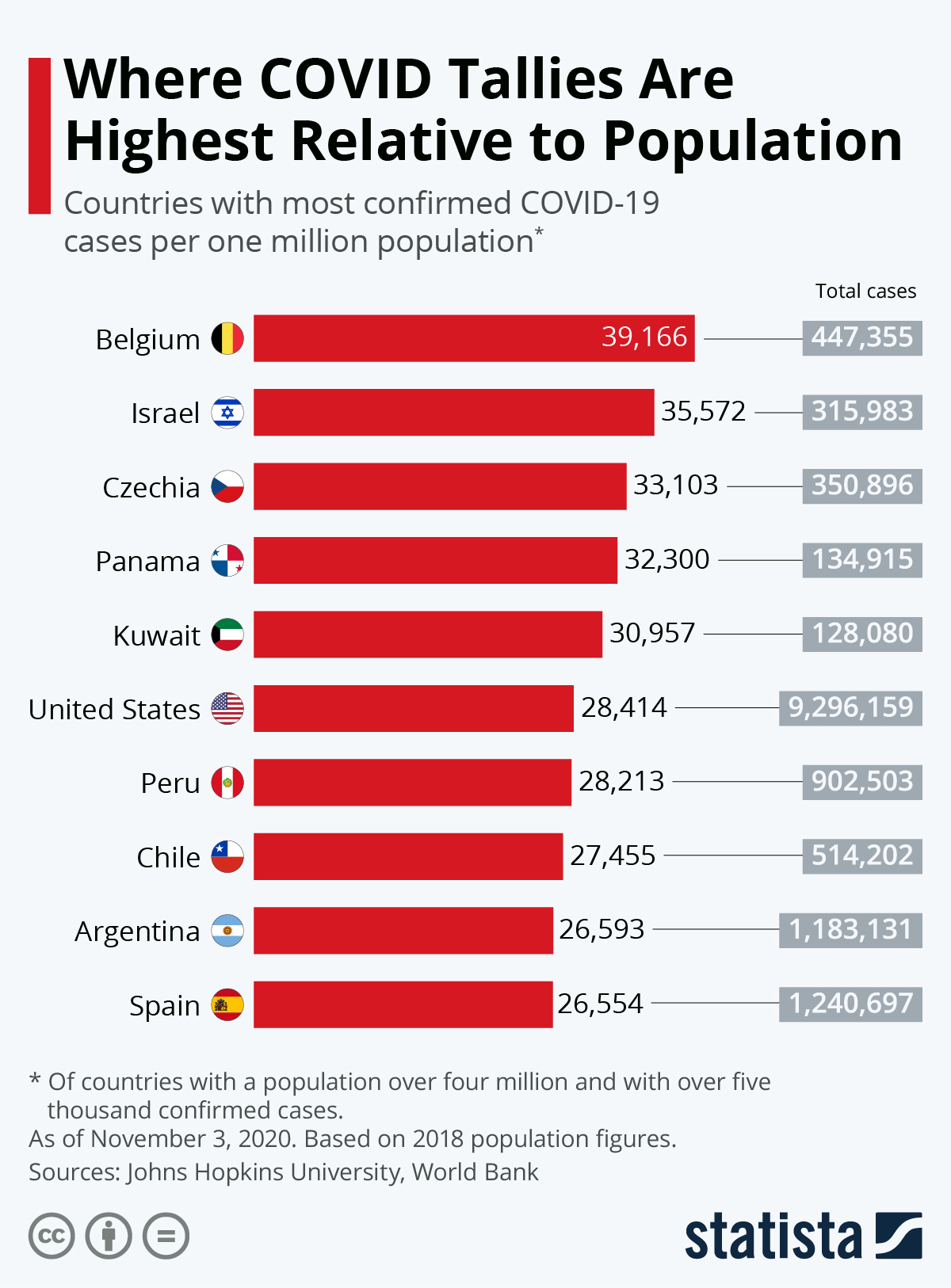
Η εξάπλωση του ιού σε σχέση με τον πληθυσμό ανά χώρα
Κατά την προσωπική γνώμη του συντάκτη, πάντως, ο αριθμός των κρουσμάτων είναι ένα παραπλανητικό μέγεθος. Μπορεί, δηλαδή, να υποδηλώνει ορθώς την εξάπλωση του ιού (πχ Ιταλία), ωστόσο μπορεί να είναι αποτέλεσμα ευρείας (σε σχέση με τις άλλες χώρες) διενέργειας των διαγνωστικών εξετάσεων (πχ Γερμανία, ΗΠΑ μετά την αλλαγή πολιτικής τους, Ελβετία). Ο αριθμός των θανάτων και των βαρέως πασχόντων ασθενών (νοσηλευόμενοι σε μονάδες εντατικής νοσηλείας) είναι πολύ πιο ενδεικτικοί. Απλώς, δεν έχουν προβλεπτική αξία, καθώς αντιπροσωπεύουν τη νοσηρότητα της τρέχουσας στιγμής και όχι του μέλλοντος.

Η γνώμη των ειδικών
Οδηγίες από την Ελληνική Πνευμονολογική Εταιρεία σχετικά με την σχετικά με τη διαχείριση ασθενούς ύποπτου ή επιβεβαιωμένου με COVID-19 σε χώρο Πρωτοβάθμιας Φροντίδας Υγείας .
Οδηγίες από την Ελληνική Πνευμονολογική Εταιρεία σχετικά με την διαχείριση κατ' οίκον ασθενούς ύποπτου ή επιβεβαιωμένου με covid-19 καθώς και την παρακολούθηση ασθενούς με covid-19 μετά τη νοσηλεία του στο νοσοκομείο.
Οδηγίες από την Ελληνική Πνευμονολογική Εταιρεία για τη χρήση μάσκας από το ευρύ κοινό. Μαζί με κάποιες επιφυλάξεις που συνοψίζονται:
Είναι σημαντικό η χρήση μάσκας να μην οδηγήσει σε εφησυχασμό και ψευδές αίσθημα ασφαλείας από το κοινό.Οδηγίες από την Ελληνική Πνευμονολογική Εταιρεία και συγκεκριμένα από τις αντίστοιχες επιστημονικές ομάδες εργασίας, με βάση τα νέα δεδομένα για τον νέο κορωνοϊό-2019 που ονομάζεται τώρα SARS-CoV-2 και για την ασθένεια που προκαλεί και η οποία ονομάζεται COVID-19, για τους ασθενείς με:
Η
λογική διαδρομή της επιδημίας στη χώρα μας και η πιθανή μελλοντική της συμπεριφορά.
Η μαρτυρία της πρώην προέδρου της Ευρωπαϊκής Πνευμονολογικής Εταιρείας και Διευθύντριας της 7ης Πνευμονολογικής Κλινικής του Νοσοκομείου "Η Σωτηρία".
Η πολύτιμη εμπειρία των Πνευμονολόγων από την Κίνα σε συνέντευξη (πρώτο μέρος και δεύτερο μέρος) προς την Ευρωπαική Πνευμονολογική Εταιρεία.
Η πολύτιμη, αλλά δραματική εμπειρία των Πνευμονολόγων στην Ιταλία...
Στις δύσκολες ώρες οι ειδικοί Πνευμονολόγοι είναι αυτοί δίνουν την μάχη στην πρώτη γραμμή, στην πρωτοβάθμια, δευτεροβάθμια και τριτοβάθμια περίθαλψη...
Στην Ελλάδα έχουμε την τύχη να έχουμε έναν ικανό αριθμό ειδικών και καλά εκπαιδευμένων πνευμονολόγων. Ας μην ξεχνάμε ότι η ειδικότητα της πνευμονολογίας περιλαμβάνει ως προαπαιτούμενο την εκπαίδευση επί 6 τουλάχιστον μήνες σε Μονάδα Εντατικής Θεραπείας. Ωστόσο, ελπίζω και εύχομαι να μην ζήσουμε τέτοιες στιγμές...
Ενημέρωση:14/3/2020
Θετικές πρωτοβουλίες (που σημαίνει ότι πλέον λειτουργούμε οργανωμένα):
- ήρθε το επιβεβλημένο από τις διεθνείς συνθήκες lockdown (αναστολή λειτουργίας χώρων συνάθροισης) από το Σάββατο 14/3/2020 και για 14 (αρχικά) ημέρες!
- το κενό περιεχομένου μήνυμα "καλέστε στο 1135" μετουσιώθηκε επιτέλους στο ουσιαστικό μήνυμα "μένουμε σπίτι" !
- εκδόθηκαν οδηγίες ως ενδείξεις εργαστηριακού ελέγχου λοίμωξης από το νέο κορωνοϊό-2019 SARS-CoV-2

- εκδόθηκαν σαφείς οδηγίες για να μην μετατραπούν οι χώροι παροχών υπηρεσιών υγείας σε επωαστήρια του κορωνοϊού SARS-CoV-2

- εκδόθηκαν νέες οδηγίες για τη θεραπεία των ασθενών με λοίμωξη από το νέο κορωνοϊό-2019 SARS-CoV-2 από την Ελληνική Εταιρεία Λοιμώξεων


Θα πρέπει να επισημανθούν μερικά σημεία επιπρόσθετα των γενικών μέτρων προφύλαξης έναντι του κορωνοϊού, τα οποία, κατά την γνώμη του υπογράφοντος, δεν είχαν τονιστεί επαρκώς μέχρι πρόσφατα:
- αποφυγή συνωστισμού στα ιατρεία και ευρύτερα στους χώρους παροχών υπηρεσιών υγείας !
- αποφυγή άσκοπης λήψης ή αποθήκευσης αντιβιοτικών !
- αποφυγή συνωστισμού στα πολυκαταστήματα ! Φαρμακεία και σούπερ μάρκετ δεν πρόκειται να κλείσουν !
- αποφυγή μη αναγκαίων πολύωρων ταξιδιών με επίγεια ή εναέρια μέσα μεταφοράς !
- σε ήπια πάσχοντες ασθενείς η καλύτερη στρατηγική είναι ο εθελοντικός κατ΄οίκον περιορισμός επί 14 ημέρες και η αυστηρή τήρηση από τους ασθενείς και τους φροντιστές των μέτρων προστασίας ! Σε αυτούς τους ασθενείς και στην ελληνική πραγματικότητα είναι άσκοπη η δειγματοληψία για λοίμωξη από SARS-CoV-2 ! Ο εθελοντικός κατ΄οίκον περιορισμός αποτελεί όχι απλώς ένδειξη ατομικής ευθύνης αλλά και το πιο σημαντικό μέτρο για τον περιορισμό της εξάπλωσης του κορωνοϊού! Βέβαια, σε ελεύθερες κοινωνίες ο κατ΄οίκον περιορισμός δεν διατάσσεται ούτε επιβάλλεται... Ωστόσο, θα πρέπει να τονιστεί στον δέοντα βαθμό από τις αρμόδιες αρχές, κάτι που δεν έχει γίνει επιτυχώς μέχρι σήμερα...
- σε περίπτωσης επιδείνωσης ασθενών με ύποπτα συμπτώματα (πυρετός-βήχας-δύσπνοια) και, ιδίως, εφόσον υπάρχει ιστορικό πρόσφατου ταξιδιού εκτός Ελλάδος ή επαφής με άλλο κρούσμα με SARS-CoV-2, επικοινωνία με τον ΕΟΔΥ στο τηλέφωνο 1135 ή με το ΕΚΑΒ για μεταφορά του ασθενούς στα νοσοκομεία αναφοράς.





.....
.....
- Τι πρέπει να γνωρίζουμε για το νέο κορωνοϊό-2019 που ονομάζεται τώρα SARS-CoV-2, και για την ασθένεια που προκαλεί και η οποία ονομάζεται COVID-19.
- Οδηγίες προς ευπαθείς ομάδες.
- Οδηγίες για μέτρα πρόληψης σε επίπεδο ιατρείων από τον ΙΣΑ
- Μύθοι για τον κορωνοϊό
- Οδηγίες για απομόνωση και παρακολούθηση κατ΄οίκον για άτομα με πιθανή λοίμωξη με το νέο κορωνοϊό
- Οδηγίες για απομόνωση και παρακολούθηση κατ΄οίκον για άτομα που ήρθαν σε επαφή με ύποπτο ή επιβεβαιωμένο κρούσμα λοίμωξης με το νέο κορωνοϊό
- Οδηγίες για απολύμανση
- Οδηγίες για σχολικές μονάδες
- Οδηγίες για πληρώματα ασθενοφόρων ΕΚΑΒ
- Οδηγίες για αστυνομικό και στρατιωτικό προσωπικό
- Οδηγίες για ξενοδοχεία
- Δελτίο δήλωσης κρούσματος λοίμωξης προς ΕΟΔΥ
- Συνοδευτικό δελτίο δείγματος προς εργαστήρια
- Ιστότοπος ΕΟΔΥ (πρώην ΚΕΕΛΠΝΟ)
- Ενημερωτικό υλικό από το Υπουργείο Υγείας

Παγκόσμιος Οργανισμός Υγείας
οδηγίες προς το κοινό
οδηγίες προς ιατρικό και νοσηλευτικό προσωπικό
χάρτης εξάπλωσης
καθημερινές αναφορές
μύθοι για τον κορωνοϊό
site WHO
Εμβόλια και φάρμακα που αναπτύσσονται για την αντιμετώπιση του ιού:
- Εμβόλια: έχουν το χαρακτηριστικό ότι βοηθούν στην πρόληψη παρά στη θεραπεία της νόσου, με το κύριο μειονέκτημα ότι απαιτείται μεγαλύτερος χρόνος για την ανάπτυξή τους, με την εξαίρεση, ίσως, όσων παρασκευάζονται με την τεχνολογία PCR-DNA.
- Φάρμακα: σε πιο προχωρημένο στάδιο μελετών βρίσκονται φάρμακα που έχουν ήδη αναπτυχθεί για την αντιμετώπιση του ιών HIV, Ebola, Zika, Marburg και Κίτρινου Πυρετού.
Η εμπειρία της Κίνας
Κέντρο Ελέγχου Λοιμώξεων της Κίνας: καθημερινές αναφορές

